
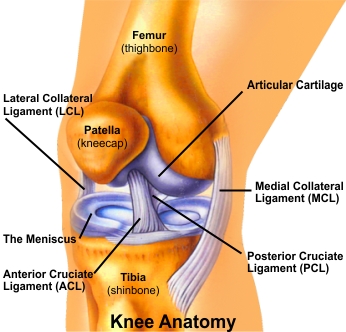
Your knee is a hinge joint where the end of the thigh bone (femur) meets the beginning of the large bone in your lower leg (tibia). A healthy knee has smooth cartilage that covers the ends of the femur and tibia. The smooth cartilage lets the surfaces of the two bones glide smoothly as you bend your knee. The muscles and ligaments around the knee joint support your weight and help move the joint smoothly so you can walk without pain. Knee Arthroscopy is a procedure that allows Dr. Riddhivardhan to look inside of your knee using an arthroscope (a slender scope that contains a lens and a light source). This enables him to obtain a clear view of the knee, diagnose, and treat knee conditions and injuries. Small incisions are made around the knee to insert the arthroscope, irrigating tool, and reparative instruments. The images are then projected on a television screen in the operating room, so that the Dr. Riddhivardhan has an enhanced view of the knee and tissues. Tradional knee surgery techniques included a large incision with an open procedure, and a lengthy hospitalization. With arthroscopy, the procedure is minimally invasive and the recovery is typically rapid. The patients either are hospitalized for one day or return home the same day. Signs that you may be a candidate for this procedure include swelling, persistent pain, catching, giving-way, and loss of confidence in your knee. On the basis of physical examination, x-rays and MRIs your Dr. Riddhivardhan will make an evaluation to determine whether you could benefit from arthroscopy. Indications for Knee Arthroscopy
- Torn or degenerate meniscus or menisci (semilunar cartilage). This can result from a twisting injury caused by either aggressive sporting activity or simply getting up from a squatting position. Also, our cartilages become brittle as we get older and therefore can tear easier.
- Articular Cartilage Damage. Sometimes, due to injury, the articular cartilage is torn compromising its shock absorbing function. Large pieces of the cartilage can float in the knee resulting in locking of the joint. These loose floating bodies can cause further wear and tear.
- Rupture of Anterior Cruciate Ligament (ACL). This is a common sporting or a trauma related injury. Once ruptured, the ACL does not heal and usually causes knee instability. In this case ACL reconstruction is required.
- Maltracking and Dislocation of the Patella (kneecap). The kneecap sits in a groove at the end of the thighbone. It is held in place by tendons on the top and bottom and by ligaments on the sides. A layer of cartilage lines the underside of the kneecap. This helps it glide along the groove in the thighbone. A problem with any of these parts in or around the knee can lead to patellar tracking disorder.
- Inflammation of the Joint Lining (synovitis). The synovium membrane is found in your knee joint. This thin membrane surrounds the inner lining of your joint and may have folds and fringes. Its main function is to create synovial fluid, which helps nourish and lubricate your joint. When part of your synovium becomes inflamed, it can cause your entire joint to swell and become tender. Knee arthroscopy can be used to remove the inflamed tissue.
After arthroscopic surgery is over, the portals are closed with sterile surgical tape and covered with a layer of gauze and crêpe bandage. The patient is then moved from the operating room to a recovery room where a nurse will monitor temperature, blood pressure and heartbeat. Before being discharged, usually several hours after your operation, you will be seen by your anaesthetist and Dr. Riddhivardhan and one of his physiotherapists. You will learn how to care for your arthroscopic portals, what activities you should avoid, and what exercises you should do to aid your recovery. At a follow-up visit (usually 10 to 14 days after the operation) Dr. Riddhivardhan will inspect arthroscopic portals, remove the skin closure and discuss the operative findings and further rehabilitation programme.